
-
1. Introduction
-
2. Translating data into action: essential components of a TB recording and reporting system
-
3. Designing an optimal information system
-
4. Recommended process of development
-
5. Resource requirements
-
6. Measuring the impact of the information system
-
References
1.2 Complexities in information systems and current landscapes
Technology advances in software development, design and performance have led to the creation of multiple systems for the collection and analysis of TB data. However, several gaps exist in terms of designing effective information systems for TB interventions (and effectively utilizing them). The information systems problem is not purely a matter of building good software. Therefore, it is important to understand the challenges involved in building, managing and using TB-related information systems:
- Heterogeneity of screening data: Screening and diagnostic algorithms vary across countries and even across projects in the same country, owing to the variation in symptoms, risk factors, and availability and use of different diagnostic tests. This makes it difficult to develop a single digital tool for TB screening and to compare and analyse screening data from different countries and projects. This limitation represents a disadvantage for creating unified reporting systems at the global level and for sharing learning experiences between settings.
- Missing data: TB indicators and required data fields are quite well-defined, but operational reasons may prevent programme staff, especially data collectors, from finding necessary data, which may not even be available (e.g. patient addresses).
- Limited analytical capacity of the end-user: Many TB programmes do not have the technical capacity to make use of the vast amounts of new (and existing) data that information systems can make available. This limited capacity represents a massive lost opportunity to apply the evidence being generated in order to make decisions on course correction around programmatic improvements.
- Multiple parallel systems: TB programmes considering electronic systems for TB recording and reporting have three options: 1) choose from pre-designed options; 2) work with an existing and often confusing array of systems that may or may not link with the existing health information infrastructure in the country, or 3) have something custom-built. Given these choices, multiple recording and reporting systems exist globally, each tailored to specific types of TB recording and reporting; each with its own strengths and limitations; and each functioning in isolation. At the global level, this leads to the issue of data heterogeneity described earlier, while at the national level, this may lead to fragmentation in data and duplication in reporting. For example, there have been cases where multiple donors have funded different systems in the same country – one for DS-TB, another for DR-TB, and to further complicate the issue, a third system for HIV – without linking the systems together. This means that the data for one HIV patient who is first notified as a DS-TB patient but is later found to have DR-TB will be split across three different systems. Many countries are using aggregate data systems like DHIS2 at the Ministry of Health (MoH) level. In such cases, any additional systems should be configured to report into the DHIS2.
- Limited ownership and accountability: The ultimate ownership of a national TB information system rests (or should ideally rest) with the NTP or with even higher agencies such as the MoH. However, there are several reasons as to why this does not happen. NTPs often do not have the capacity to determine what would work best for their context from an information systems standpoint. Technical IT capacity within NTPs is often limited, leaving them at the mercy of private providers for even simple modifications and maintenance tasks. KNCV’s Digital Health Assessment approach [4] (see Figure 2 and Section 7) addresses this issue by working closely with governments to assess existing information systems and to identify any opportunities and gaps along the patient care pathway that can be addressed by digital solutions (5).
- Resource issues: Donors, programme managers and implementing groups often fail to realize that an information system for a large intensive case-finding programme requires a significant investment in time, human resources, and capital – an investment that goes beyond simply developing and deploying a system and buying phones or computers for data entry and reporting. Information systems are long–term investments and will usually undergo multiple iterations and enhancements before they can pay back dividends in the form of efficiencies from digital data collection and analysis and improved treatment outcomes. Success requires programme staff to be actively involved in the design and implementation of information systems. If programmes do not budget and plan adequately for these systems, this shortsightedness can have negative impacts ranging from simple under-utilization of the system to complete failure of the information system initiative.
Overcoming these challenges requires thoughtful approaches, some of which are discussed in this document.
Figure 2. Example of a completed digital health activities framework
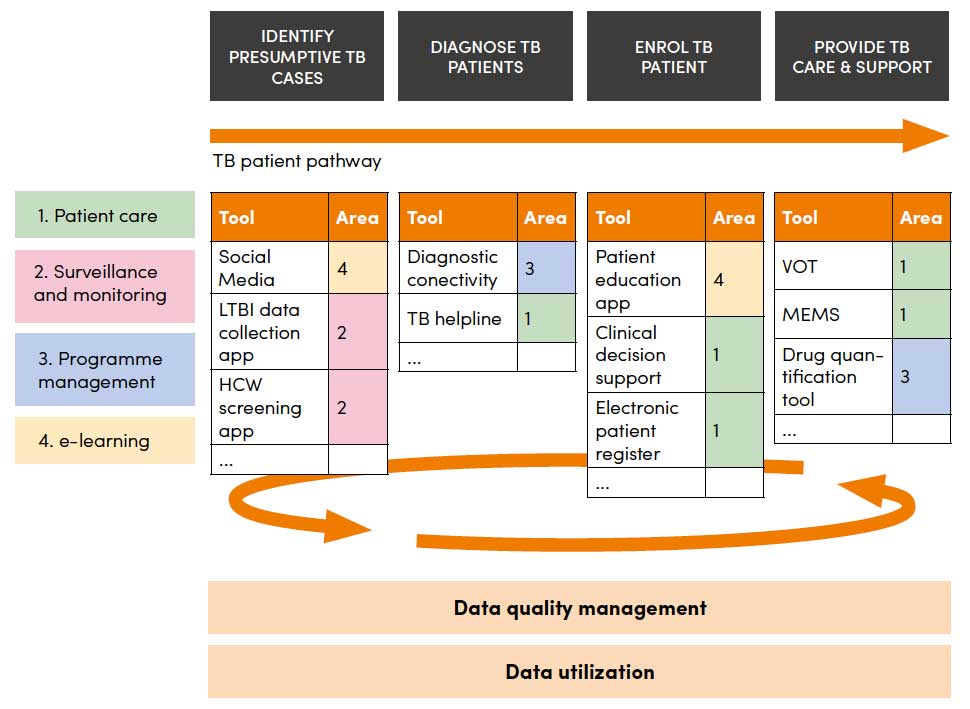
HCW: health-care worker; LIMS: laboratory information management systems;
LTBI: latent tuberculosis infection; MEMS: medication event monitoring system;
VOT: video-supported treatment for TB
Source: WHO’s Handbook for the use of digital technologies to support tuberculosis medication adherence (6)