
-
1. Introduction
-
2. Translating data into action: essential components of a TB recording and reporting system
-
3. Designing an optimal information system
-
4. Recommended process of development
-
5. Resource requirements
-
6. Measuring the impact of the information system
-
References
Introduction: Why invest in information systems for TB?
Finding and treating people with tuberculosis (TB) is a multi-step process involving awareness generation, prevention, screening, testing, diagnosis, treatment initiation, multiple follow-ups and finally a successful treatment outcome. This, by necessity, involves recording data at each step of the process, not only to track patients’ progress through the TB care cascade, but also to understand key indicators of programme performance that can inform the decisions of programme managers and policy makers.
Various types of data systems can be used at different points in the TB diagnosis, treatment and care cascade, for example:
- Laboratory information management systems (LIMS)
- Patient surveillance systems
- Pharmacy management systems
- Adherence tracking systems
- Notification systems
All of the above have the potential to be relevant for the management of TB patients. Throughout this document, the term “information system” refers to any system that is used to transfer data relevant for TB programme management.
There is an acute need for adequate data management in TB programming. In the mid-1990s, the World Health Organization (WHO) rolled out a standardized system for paper-based recording and reporting of TB patient data, from diagnosis to treatment outcome. This system, which includes geographical, administrative and quality control information, is a key element of the WHO DOTS (directly observed treatment, short-course) strategy, as well as its successor, the Stop TB Strategy (1). By the mid-2000s, more than 99% of the world’s reported TB cases were being recorded and reported in countries that had adopted the WHO-recommended system. Largely due to the implementation of this system, TB data are comparable across many thousands of treatment facilities worldwide. The standard datasets that countries use to provide data to WHO allow for reporting on the global TB epidemic and progress in TB care and prevention (2).
Information systems supported by mobile technologies have the potential to enable programme implementers to collect patient data from different sources and locations. Data can be made easily accessible in a case record format, and used for faster, easier reporting and analytics.
Information systems can benefit programmes that are focused on finding the missing people with TB by improving treatment linkages for those diagnosed and by improving reporting of those who may have been diagnosed and treated but not notified. Bringing these individuals under notification generally has the benefit of ensuring access to national minimum standards of diagnosis, treatment and investigation, and improving the completeness of data for epidemic response planning. Below are some examples of data systems currently being used in TB control programmes:

- eTB manager: a desktop-based tool for managing multiple layers of TB programme data on TB patients, medicines, laboratory testing, diagnosis, treatment, and outcomes.[1]
- NIKSHAY: India’s web-based solution built to record notifications for the country’s TB and multidrug-resistant (MDR-) TB patients, and to use these data for patient monitoring and research.[2]
- QuanTB: a quantification and early warning system for TB medicines, aimed at improving procurement processes, ordering and supply planning.[3]
DHIS2 (District Health Information System 2): used as an aggregate data system at the national level in more than 40 countries in Africa, Asia and Latin America.
Compared to the paper-based systems currently still in use in many settings, well-designed digital information systems, including the ones cited above, are faster, more efficient and more secure. Box 1 summarizes the potential benefits of moving from a paper-based to an electronic system (3).

Large amounts of information notwithstanding, data are frequently underutilized for programmatic course correction for a variety of reasons, such as the following:
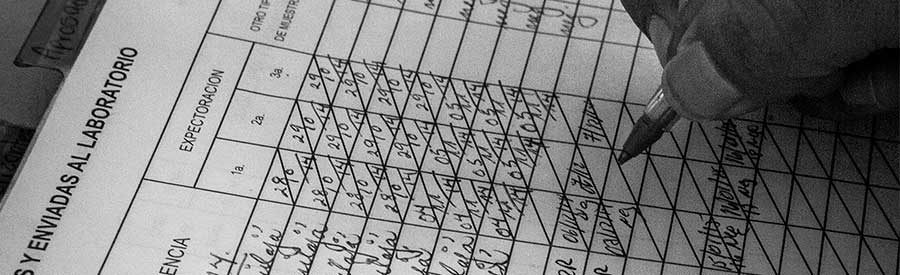
- Paper-based systems continue to be a key method of information sharing (sometimes in a hybrid setting, with data being shared via both paper-based and electronic routes); this type of system may not lend itself to quick aggregation, analysis and data-driven decision-making in the short term (see Figure 1 for an example).
- Sometimes, even when electronic systems have been set up, workflow changes at implementation level do not change to incorporate the usage of electronic systems.
- Project protocols often require data to be aggregated at the end of a quarter (or even a year), which does not lend itself to agile decision-making.
- Programme designs often do not include protocols for data utilization.
Figure 1. Example of paper-based reporting system in Georgia
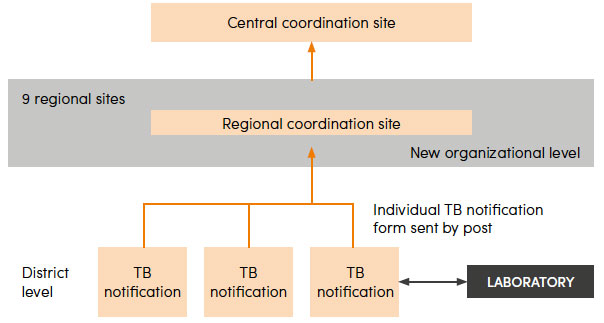
Note: TB case information in Georgia is collected on paper forms at the district level and sent by regular mail to the regional level where it is electronically recorded (3).